
This letter exchange between Judit and Alissa examines efforts to achieve SDG 3—good health and well-being—in Belgium, Morocco, and Niger. Through personal experiences and critical discussion, they address healthcare systems, social inequalities, mental health, and policy challenges, highlighting the importance of combining individual responsibility with strong public systems to improve access and quality of care for all.
LETTER 1
JUDIT STEVERLYNCK
Hello!
I am Judit Steverlynck, a Belgian student at University of Antwerp. I am studying (bridging/switching program for) Master Social Work after I accomplished (Professional Bachelor) Work and Organizational Applied Psychology. Further I volunteer in a youth movement: KSA; it’s a very typical youth movement here in Belgium. We make activities for children every saturday, a summercamp in july(between 6 – 18 years old) and we organise couple events to finance the summercamp. Further I really like to read, bake and being creative (painting, puzzles, Lego, etc.). What about you?
For this project we both chose the SDG 3: Ensure healthy lives and promote well-being for all at all ages.
For me personally, I find this SDG very important. I truly believe that the mind and the physical body are connected to each other. A dutch saying: “Een gezond geest in een gezond lichaam”, which is a famous quote that comes from Latin: “Mens sana in corpore sano” (By Juvenalis). This connection between mind and body really give quality to your life. Maybe throughout this belief and the quote, this might be an (underlining) reason why I study (Work and Organizational) applied psychology and now study for Master Social Work. Understanding the mind (psychology) and making sure everyone (even the vulnerable people (in society) can get access to a healthy life (through institutions: hospitals, sportcenters, etc).
When I think about SDG 3 in Belgium, I immediately think of a very typical Belgian system: social security. Social security is a public system that protects people against loss of income and provides basic provisions in case of illness, unemployment, old age, or other vulnerable situations. It’s a system intended to guarantee income or care for individuals or families who are temporarily or permanently unable to provide for their own livelihood (for example: unemployment, illness, disability, retirement, etc.). It is a system acting as a kind of safety net to prevent poverty. Social security is provided through social insurance (with premium payments) and benefits such as unemployment benefits, health insurance, disability benefits, etc., but also through social provisions by the government if one is unable to do so oneself, such as child benefit (in dutch: kinderbijslag/groeipakket) and social assistance (a form of poverty reduction by the government and a premium-free and conditional benefit based on the ‘means-tested’). This social security system makes it possible that all people (young, old, rich, poor, etc.) have access to healthcare. The low cost, reimbursement (in dutch: terugbetaling), good accessibility, low-threshold aid services/care provision (in dutch: laagdrempelige hulpverlening), etc). That’s why I’m in favour and proud Belgian; because of our welfare system and social security. And because of that system, I am also one of the few Belgian that is happy to pay taxes to get a possibility to live a healthy good life in return.
To fulfil this SDG and the social security system (in Belgium), we work with government institutions and also with (quite a lot) low-threshold aid services/primary care. Low accessible care providers like nurses, remedial educators, psychological consultants, Social Workers, etc. These care providers have a narrow relationship/connection with the government, which this can be good and bad at the same time. The government can finance these people and organisations but at same time can pressure them. This pressure is happening right now in Belgium with the new government (since 2025); where they give less money/ less grants (in dutch: subsidies) to the social sector of society. With this, it puts more pressure on the organisations to do their qualitative work with less resources; that is the pressure. Here we can ask question to ourself: what can we do with this pressure put on careworkers/on low accessible aid services (like Social Workers) to still do qualitative work for people in society?
Withing the aid services/ care provision (in dutch: hulpverlening), we also talk about mental health care. Through my eyes I could say we improved, especially if we compare it to couple years ago. Since a long time/couple years ago, mental illness was not always believable as a real sickness. So viewing through this point of view, I feel I could say we improved. An example that the mental illness burn-out was 10-15 years old seen as a ‘laziness’, and now as ‘mental illness/ energy problem’. With this view point, I believe we’re going to make improvement; quality takes a while.
I could say we’re in a ‘between-time’; time to still work on better improvements, but we also improved. What do we do in this ‘between-time’? Do we just wait our time and keep having small steps towards improvement to a better quality of the services? Like an example here in Belgium with a campaign they recently announced. The campaign “Kom van dat gat af” (“Get off that (lazy) butt”) is organised by the government and semi-governmental organisation VRT (Flemish Radio & Television Broadcasting Organization). It’s a campaign to get people to sit less longer, be more active and move throughout the day; to in long-term improve a better healthy life-style. Specifically this campaign is focused on 1 day (April 2nd), were my question is: why only make it one day and not a long-term campaign were you find tips and tricks to fulfil the goal. Or do you not wait and give a not qualitative service to people? Like the problem here in Belgium with very long waitlist or no good referral to quality help with to services of Mental Health services/hospital.
Besides these formal (government) institutions, I also personally believe that little things you do yourself can be good to fulfil this SDG. Little things like: ‘How do I organise my day? Will I go have a workout or have a run before I have to go to work/school, or will I rather stay in my bed and sleep’. These little things ‘choices’ also support whether you have a healthy lifestyle or not (to fulfil SDG 3).
We do have to keep in mind that we need both: our little things ‘choice’ in daily life AND the formal (government institutions). We need both to decide how you organise your day, how you organise school (system) and work (system)?
In Belgium is the labormarket very strongly around the knowledge economy and bureaucratism. With this it means that jobs with a lot of knowledge and diploma requirements are higher valued, promoted and rewared than the practical (technical) jobs. A very simple example to illustrate this: a professor in University gets more paid then a cleaner or plumber. Even though because of knowledge economy and bureaucratism we see ‘knowledge jobs’, the practical (technical) jobs are also essential and important. But these jobs are less attractive to do due to the low status, low wage and low valuation. The need that these practical jobs are essential, I also see in discussions (and frustration) on Facebook. But in my opinion you need both: the ‘knowledge jobs’ and practical (technical) jobs in society. It could be logical to make the pay more equal, make the wage gap smaller and/or make the practical jobs more attractive and ‘normal’ to choose as a career choice. This is what never sits right with me.
Reason why I deviate from the distinction between practical and knowledge office jobs is, because this also indirectly affects SDG 3; it’s a “choice” of how you organise your day/system to whether you have a healthy lifestyle. In a knowledge office 9-to-5-job there is a lot of sitting during the day, time pressure; which makes it harder to organise your day to have a fully qualitative healthy day were you cook and eat healthy and do a sport.
Even with this society organising this way (knowledge economy and bureaucratism), I could see development in Belgium toward the SDG 3 within the lines of this kind of organising society.
- The school system (from elementary to high school) (still) rely on an 8 hours “sit and listen” model, so to still fulfil SDG 3 they add tools/gadgets that encourage more movement during the day. Tools/gadgets like wobbly chairs, exercise balls, bicycles under school desks, standing tables, etc. During the years become more common to make students be more active, less sitting all day.
- The implementing of these gadgets/tools was also an attempt into the workplace, but this mostly appears in (semi-)government organisations. A likely reason is that they have more funding, facilities like sport rooms, lower work pressure, making such initiatives/facilities easier to implement.
Overall, you see that Belgium tries to fulfil this SDG 3 and give pretty good access of aid services/care provision(by the social assistance system) to make sure everyone (all people, all ages) have a good, healthy lives and well-being. But you can always improve it! Belgium makes progressive to work on it.
How does your country Morocco try to fulfil the SDG (Sustainable Development Goal) 3: Ensure healthy lives and promote well-being for all at all ages?
Greetings,
Your Global Pen Friend
Judit Steverlynck
LETTER 2
ALISSA CHAIBOU SOULEY
Bonjour Judit,
Merci encore pour ta lettre très intéressante. J’ai vraiment apprécié découvrir ton parcours, ton engagement ainsi que ta vision de l’ODD 3. J’ai particulièrement aimé ta réflexion sur le lien entre le corps et l’esprit, avec laquelle je suis totalement d’accord.
Pour me présenter un peu plus, je m’appelle Alissa Chaibou Souley, je suis une étudiante nigérienne en Master 1 de Management des Organisations, Économie Sociale et Solidaire et Innovation Sociale (MOESSIS) à la Faculté des Sciences Juridiques, Économiques et Sociales d’Oujda, au Maroc. Je suis également titulaire d’une licence en sciences économiques et gestion obtenue à la FSJES de Meknès.
Je suis passionnée par le cinéma, la cuisine et les voyages. J’ai également été engagée dans des associations étudiantes au Maroc. J’ai occupé le poste de trésorière et chargée des affaires culturelles au sein de l’ANEM (Association des Nigériens Étudiants et Stagiaires au Maroc – Meknès), puis chargée de l’organisation et des affaires culturelles au sein du CESAM (Confédération des Élèves, Étudiants et Stagiaires Africains Étrangers au Maroc – Meknès). En tant qu’étudiante étrangère, ces expériences ont été très enrichissantes pour moi, car elles m’ont permis de représenter ma culture tout en découvrant celles des autres.
Pour répondre à ta question, le Maroc essaie de réaliser l’ODD 3 principalement à travers la généralisation de la couverture sanitaire universelle, appuyée par des réformes structurelles du système de santé.
Depuis 2021, le Maroc a lancé un chantier majeur visant à étendre l’Assurance Maladie Obligatoire (AMO) à l’ensemble de la population. Ce système permet aux assurés de bénéficier d’une prise en charge d’une partie importante des frais de santé, notamment les consultations médicales, les médicaments, les hospitalisations et certains soins spécialisés. L’objectif est de réduire les dépenses directes des ménages et de garantir un accès équitable aux services de santé.
Parallèlement, l’ancien Régime d’Assistance Médicale (RAMED), qui était destiné aux populations les plus vulnérables, a été intégré dans ce nouveau système à travers un mécanisme unifié. Cette intégration vise à renforcer la solidarité nationale en assurant une meilleure couverture des personnes en situation de précarité. Désormais, ces populations peuvent accéder aux soins dans des conditions plus équitables, tout en étant protégées contre les risques financiers liés à la maladie.
Grâce à ces réformes, plus de 35 millions de Marocains sont aujourd’hui couverts, soit environ 86,5 % de la population. Cette avancée a permis de réduire significativement les paiements directs des ménages et d’améliorer l’accès aux soins. En parallèle, le Maroc investit également dans le développement des infrastructures de santé, notamment dans les zones rurales, afin de réduire les inégalités territoriales et d’assurer une meilleure répartition des services médicaux.
Cependant, malgré ces progrès importants, plusieurs défis persistent. Une partie de la population n’a pas encore un accès effectif aux soins, en raison de disparités régionales, de certaines contraintes administratives et d’un manque de ressources humaines dans le secteur de la santé. Cela montre que la réussite de l’ODD 3 ne dépend pas uniquement des réformes adoptées, mais aussi de leur mise en œuvre concrète et de leur efficacité sur le terrain.
Par ailleurs, en ce qui concerne l’ODD 3 dans mon pays d’origine, le Niger, des efforts sont également réalisés, mais les défis restent plus importants. Le Niger met en place plusieurs politiques visant à améliorer la santé des populations, notamment à travers des programmes de santé maternelle et infantile, la gratuité de certains soins pour les femmes enceintes et les enfants, ainsi que des campagnes de vaccination à grande échelle.
Dans ce cadre, des organisations internationales comme l’UNICEF jouent un rôle essentiel. Elles soutiennent le gouvernement nigérien en fournissant des vaccins, en renforçant les systèmes de santé, et en développant des programmes de nutrition et de prévention des maladies. L’UNICEF intervient également dans la sensibilisation des populations et l’amélioration de l’accès aux soins de base, notamment dans les zones rurales.
Malgré ces efforts, le Niger fait face à de nombreuses difficultés, telles que le manque d’infrastructures sanitaires, le déficit en personnel médical qualifié et les inégalités d’accès aux services de santé. Ces contraintes rendent plus complexe la réalisation de l’ODD 3, même si des progrès sont observés grâce à la collaboration entre l’État et les partenaires internationaux.
Je partage également ton point de vue sur l’importance des actions individuelles. Les politiques publiques sont essentielles, mais les choix du quotidien, comme l’alimentation, l’activité physique ou la gestion du stress, jouent aussi un rôle important dans le bien-être et la santé globale.
Enfin, j’ai trouvé ton analyse du système belge très intéressante, notamment le rôle de la sécurité sociale et les défis liés à la pression sur les travailleurs sociaux. Cela montre que même les systèmes les plus avancés doivent continuer à évoluer.
J’aimerais beaucoup en savoir plus sur ton expérience en Master et sur le type de carrière que tu envisages dans le domaine du travail social.
Au plaisir de te lire bientôt,
Bien à toi,
Alissa Chaibou Souley.
LETTER 3
JUDIT STEVERLYNCK
Hello Alissa,
First of all, most of the french I actually could understand it without a translator. But at some point were the letter got more serieus into the topic, I had to get a translator. But proud of myself to mostly understand it, haha! It’s nice to read who you are and what you like, what a coincidence that we both like to cook and travel. I find it also nice that you got the foreign experience to represent your own culture and get to know other cultures. That’s always an enrichment. For me personally, I believe that everyone should have a chance in their life to meet with other cultures, and other people meet with your own culture. I believe in this, because I see the enrichment since I also did an exchange year to Canada where I did my grade 12 again. Mostly to improve and learn English, but learning different cultures was also an enrichment.
Nice to read that you liked my explanation of the health care system and social security/ social assistance system in Belgium, because it is quite a complicated system; even some politicians sometimes say this haha. Mutual it was very interesting to read about how Morocco and Niger try to fulfill this SDG 3; access to healthcare for everyone in the country. Also nice to read that we both agree on some things, like that there is a connection between corps and mind (“Mens sana in corpore sano”, by Juvenalis) and the importance of individual actions/all-day choices to have a good healthy life; both physically and mentally. It’s important, but not to forget that it’s not the only thing. It’s best to have a mixture of the individual actions/choices and the government support to have a healthy, qualitative life.
It was very nice to read the situation in Morocco, I do have some questions about it; so I could understand it completely. Morocco has an general implementation of universal health care, supported by structural reforms of the health system. It’s since 2021 there’s also a mandatory health/sickness insurance for the entire population; which is comparable to the social security and social insurance here in Belgium. I was just wondering if there is a connection why this got accomplished in 2021, after Covid 19. Did the pandamic of Covid 19 played a role to get this mandatory health/sickness insurance for the whole population?
Further you said that Morocco works with RAMED system. Which seems comparable to the social assistance here in Belgium, just more focused on the medical assistance. The social assistance in Belgium is to make sure everyone; even the vulnerable people; could have a healthy, qualitative life: housing – food – medical stuff, …). Just were I understand it, the RAMED system makes sure that the whole population and mostly the vulnerable people have access to health care and medical insurance. As you said: “Because of this sysem most vulnerable people gain access to healthcare under equal conditions, among other things, and are protected against the financial risks of illness”. Just a very critical question from me: does this system makes a difference in tools, acces, etc. between the people and the more vulnerable ‘poor’ people, if so how?
It was very interesting to read some statistics, it maded it more clearer. Like where I can see that the reforms really made sure a lot of the population has access to healthcare. Ofcourse there are always issues and challenges; but with these statistics it seems like quite a great growth. You even mention some challenges like territorial inequalities and deficit of the (healthcare) staff.
- The challenge of the territorial inequalities, where I wonder if it’s that big difference of access to healthcare when you live in a city or rural area? Or how can I understand these territorial inequalities? You even mention that some territorial regions sometimes don’t have any access, could you tell me how this come, is it too far away or difficult to reach, etc.?
| To address that challenge in Belgium or more like Flanders, there is a division of different zones for first aidcare, like you see in the picture. It’s a network of first-line care providers of police, ambulance, social workers, psychologist, doctors, etc. are distributed across zones throughout Flanders and Brussel. In total there are 59 in Flanders and 1 in Brussel. The zone is just large (or small enough) so that the emergency services can certainly provide (quick) assistance on site within 10-20 minutes. | 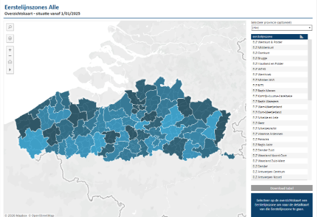 |
- The challenge of deficit of the (healthcare) staff, where I immediately recognize this challenge in Belgium too. In my last letter I mention the deficit of practical jobs; like nurses, plumber, elektrician, baker, etc. The jobs were you don’t necessarily need an academic (not professional) diplom for. For us, the reason of this deficit as I mention earlier could be that Belgium is focusing on knowledge economy, where only the academics get rewarded and paid good and not the practical jobs. Practical jobs have low rewards and low wages, where not many people want to take those jobs. This knowledge could be (one of) the reason here in Belgium/West-Europe for the deficit of the (healthcare/practical) staff. I am curious what you think might be the reason there is a deficit of (healthcare) staff in Maroco?
Very interesting to read also more about your birthcountry: Niger, to see similarities and differences between Niger, Marocco and Belgium. I could say that they are quite good working on fulfilling this SDG 3 in Niger, but it’s mostly from an universal organisation (like UNICEF). Well, I am assuming; where I could be wrong; it’s mostly from UNICEF, where I am curious to know whether the government of Niger has their say in it; and how much and how the dynamic/relation is between Niger government and the universal organisation working on SDG’s. Further I am also curious how the government of Niger is thinking about fulfilling SDG 3 for everyone, the whole population?
Lastly I will answer your question to know more about my master’s program Social Work, and which career I want to go for in the social sector/in my careerlife.
The master program Social Work is further building on the bachelor social work, but since the social work practice field is large and diverse, any study in social pedagogical direction could follow this master. Just like me, with my bachelor of applied work and organizational psychology. With this master, they teach and train you primarily to become a social researcher and policymaker. With this position you can do a social research, brainstorm for possible solutions or actions and propose it to the political policy. We delve into the social problems playing out in the world and in the person/client’s lifeworld. Furthermore, we’re trained to be (academic) researchers, to conduct (academic) social research in the social sector and in the world/society where these social problems play out. Social problems like: gender inequality, poverty, climate change (inequalities), discrimination and so on. This academic research can then be used and read by politicians and/or policy makers, and find solutions and/or change, make new rules where the social problems can be tackled. Not solved, because these social problems are often ‘wicked problems’ that can’t be solved.
The social problems were I’m personally more leaning to work later in my career with, is gender discrimination, mostly in work context, but overall. Gender discrimination where also the positive discrimination in the work context is included. This aligns closely with my bachelor’s degree in Applied Work and Organizational Psychology. Further I’m also interested to make sure everyone; all young girls, women, and men; feel safe, in the city, town and nightlife. One reason why I’m interested in the safety aspect is, that I wrote my Bachelor thesis on this theme. For this Bachelor these, 4 others and I developed a social enterprise to promote a sense of safety among young people in nightlife. Those 2 big themes of social problems are the one where I really want to work on in my career; if possible. A career where I hopefully can conduct social research myself with a team, and than use my creative brain to brainstorm for some suggestions, advice or even solutions to tackle this social problem and suggest to the politicians and the government. For my career, I hope that I can do both: do the social research and use my creative brain to make suggesions, advice and solutions. Just like I somewhat did with the social enterprise for my Bachelor thesis.
What do you hope that your career can look like?
Greetings,
Your Global Pen Friend
Judit Steverlynck
LETTER 4
ALISSA CHAIBOU SOULEY
Bonjour Judit Steverlynck,
Merci beaucoup pour ta lettre très réfléchie et pour toutes tes questions. J’ai vraiment apprécié lire ton point de vue ainsi que les comparaisons que tu as faites entre la Belgique, le Maroc et le Niger. Tes remarques m’ont permis de réfléchir plus profondément aux défis liés à l’accès aux soins de santé et à la réalisation de l’ODD 3.
Concernant ta première question sur le lien entre la Covid-19 et la généralisation de l’assurance maladie obligatoire au Maroc, je pense effectivement que la pandémie a joué un rôle très important. Même si les réformes de la couverture médicale existaient déjà avant la crise sanitaire, la pandémie a révélé les limites du système de santé marocain, notamment les inégalités d’accès aux soins et la vulnérabilité des personnes qui n’avaient aucune couverture médicale. Cela a accéléré la volonté politique de généraliser la protection sociale. En 2021, le Maroc a lancé un grand projet royal visant à étendre l’Assurance Maladie Obligatoire (AMO) à l’ensemble de la population, y compris les travailleurs indépendants et les personnes du secteur informel. L’objectif était de renforcer la résilience sociale et d’éviter que les populations vulnérables soient exclues du système de santé lors des crises sanitaires.
Pour mieux comprendre le système marocain, il faut savoir que la Couverture Médicale de Base reposait sur deux mécanismes : l’AMO, qui est contributive pour les salariés et les personnes ayant des revenus, et le RAMED, destiné aux populations pauvres et vulnérables. Avant la création de ces dispositifs, seulement environ 16 % de la population marocaine bénéficiait d’une couverture médicale, ce qui créait d’importantes inégalités sociales et territoriales. Le RAMED a donc été conçu comme un système d’assistance médicale permettant aux personnes défavorisées d’accéder gratuitement aux hôpitaux publics.
Cependant, comme tu l’as très bien souligné, le système RAMED présente plusieurs limites dans la pratique. Théoriquement, il vise à garantir l’égalité d’accès aux soins, mais dans la réalité, les différences restent importantes entre les personnes disposant de moyens financiers et les plus pauvres. Les hôpitaux publics sont souvent surchargés, les délais d’attente sont très longs, certains équipements médicaux manquent et les patients doivent parfois acheter eux-mêmes des médicaments ou réaliser des analyses dans des laboratoires privés. Cela crée une forme d’inégalité indirecte : les personnes ayant des ressources financières peuvent contourner les lenteurs du système public en payant des soins privés, tandis que les plus pauvres restent dépendants d’un système sous pression. Des recherches réalisées dans des hôpitaux universitaires marocains montrent même que de nombreux bénéficiaires du RAMED ont dû payer des médicaments ou des examens malgré leur statut d’assistance médicale.
Les inégalités territoriales constituent également un défi majeur au Maroc. Les grandes villes comme Casablanca ou Rabat disposent d’infrastructures modernes, d’hôpitaux spécialisés et d’un nombre plus élevé de médecins. En revanche, plusieurs régions rurales ou éloignées souffrent d’un manque important d’équipements et de personnel médical. Certaines populations doivent parcourir de longues distances pour atteindre un centre de santé ou un hôpital spécialisé. Cela est particulièrement difficile dans les zones montagneuses ou isolées où les moyens de transport sont limités. Les retards dans la prise en charge médicale peuvent alors aggraver l’état des patients. Les statistiques montrent d’ailleurs qu’une grande partie des médecins travaillent dans les zones urbaines, alors qu’une proportion importante de la population vit encore dans les zones rurales. Ces déséquilibres créent ce qu’on appelle parfois des « déserts médicaux ».
Le manque de personnel de santé au Maroc est lié à plusieurs facteurs. Beaucoup de médecins préfèrent travailler dans les grandes villes ou à l’étranger où les salaires, les conditions de travail et les perspectives de carrière sont plus attractifs. Les hôpitaux publics souffrent souvent d’un manque de ressources humaines et matérielles, ce qui augmente la charge de travail du personnel soignant. Les jeunes médecins hésitent aussi à exercer dans les régions rurales à cause de l’isolement, du manque d’équipements et des difficultés de vie quotidienne. Pour répondre à ce problème, le gouvernement marocain essaie aujourd’hui d’augmenter le nombre de professionnels formés et de mettre en place des incitations financières pour encourager les médecins à travailler dans les régions défavorisées. Je te mets également quelques documents qui pourront encore davantage t’aider à mieux comprendre les sujets abordés dans cette lettre, notamment le système de santé au Maroc, les inégalités d’accès aux soins au Maroc. J’espère qu’ils pourront enrichir ta réflexion autant qu’ils ont enrichi la mienne :
J’ai également trouvé très intéressante la manière dont la Belgique, et particulièrement la Flandre, a organisé les zones de premiers secours afin de garantir une assistance rapide aux populations. Je pense sincèrement que cela pourrait être une très bonne solution si le Maroc adoptait un système similaire, surtout pour réduire les inégalités d’accès aux soins entre les zones urbaines et rurales. Une meilleure répartition des services d’urgence, des professionnels de santé et des infrastructures médicales pourrait aider de nombreuses populations vivant dans des régions éloignées à recevoir des soins plus rapidement et dans de meilleures conditions.
Concernant le Niger, tu as raison de dire que les organisations internationales jouent un rôle très important dans la réalisation de l’ODD 3. Des institutions comme UNICEF, le Programme des Nations Unies pour le développement, la Banque mondiale ou encore la Banque africaine de développement participent activement au financement et à la mise en œuvre de projets liés à la santé, à la résilience et à la lutte contre la pauvreté. Cependant, le gouvernement nigérien reste également impliqué. Par exemple, le programme de coopération du PNUD 2019-2021 a été élaboré en partenariat avec le gouvernement nigérien, les organisations de la société civile et plusieurs partenaires internationaux afin de renforcer la gouvernance, la résilience et l’accès aux services publics essentiels, notamment dans les zones rurales et frontalières.
Le Niger fait face à de nombreux défis structurels : pauvreté, insécurité, changements climatiques, faibles infrastructures et croissance démographique rapide. C’est pourquoi les partenariats internationaux sont essentiels. Le gouvernement cherche néanmoins à améliorer progressivement les services publics, renforcer les capacités locales et favoriser l’accès aux soins pour les populations les plus vulnérables, particulièrement les femmes et les jeunes.
Enfin, Concernant ma future carrière, je suis actuellement au Maroc où j’étudie dans un master appelé Management des organisations, économie sociale et solidaire et innovation sociale. Ce programme combine le management, l’innovation sociale et le développement territorial, ce qui me permet de réfléchir aux problèmes sociaux tout en cherchant des solutions concrètes et durables. Ce que j’apprécie particulièrement dans ce master, c’est qu’on n’apprend pas uniquement en théorie sur les bancs de l’université, mais aussi directement sur le terrain. Pendant notre formation, nous avons participé à plusieurs ateliers sur l’innovation sociale et le développement durable, où nous avons notamment appris l’importance du tri des déchets et de la gestion durable des ressources.
Nous avons également effectué des sorties de terrain très enrichissantes. Par exemple, nous avons visité une décharge publique et une station de valorisation des déchets, où nous avons découvert concrètement le principe de l’économie circulaire. J’ai trouvé cela très impressionnant de voir comment certains déchets peuvent être transformés en électricité et même contribuer à la production d’eau traitée. Cette expérience m’a permis de comprendre que les déchets peuvent aussi devenir une ressource utile lorsqu’ils sont bien gérés.
Nous avons aussi participé à des visites dans des salons d’artisanat et de commerce où nous avons rencontré plusieurs coopératives locales, composées principalement de femmes. Ces coopératives travaillent dans la production, la valorisation et la promotion des produits locaux. Ces rencontres m’ont beaucoup inspirée, car elles montrent comment l’économie sociale et solidaire peut contribuer à l’autonomisation des femmes, à la création d’emplois et au développement des communautés locales. Je trouve donc ce master très intéressant parce qu’il nous permet non seulement d’acquérir des connaissances académiques, mais aussi de comprendre les réalités sociales et économiques directement sur le terrain.
Après ce master, j’hésite encore entre deux possibilités. La première serait de poursuivre un doctorat en entrepreneuriat social afin d’approfondir mes recherches sur l’innovation sociale, le développement économique et les projets à impact social. La seconde possibilité serait de commencer directement une carrière professionnelle dans un domaine lié à mon master afin d’acquérir une expérience pratique sur le terrain, notamment dans la gestion de projets sociaux ou le développement local. Pour le moment, je réfléchis encore à ce qui serait le meilleur choix pour mon avenir.
Plus tard, j’ai aussi un projet entrepreneurial qui me tient énormément à cœur. J’aimerais ouvrir un grand magasin spécialisé dans la vente d’emballages dans mon pays d’origine, le Niger. Mon objectif ne serait pas seulement commercial. Je voudrais aussi que ce projet ait un impact social en créant des emplois pour des personnes proches de moi qui n’ont pas d’opportunités professionnelles. Dans beaucoup de pays africains, le chômage touche fortement les jeunes, et j’aimerais pouvoir contribuer, même modestement, à améliorer cette situation grâce à mon futur projet. Je pense que mes études actuelles en économie sociale et solidaire influencent beaucoup cette ambition, car elles m’apprennent qu’une entreprise peut aussi avoir une mission sociale et contribuer au développement de sa communauté. J’espère sincèrement pouvoir réaliser ce projet un jour.
j’ai beaucoup apprécié ta vision de ta future carrière. Je trouve que la recherche sociale et la réflexion créative sont des domaines très intéressants et très importants pour le développement de la société. Les personnes capables d’analyser les problèmes sociaux tout en proposant des solutions concrètes et innovantes peuvent réellement contribuer à améliorer la vie des populations et influencer positivement les politiques publiques.
Je te souhaite sincèrement de réussir tous tes objectifs et tes projets professionnels. Et qui sait, peut-être qu’un jour je verrai ton nom apparaître dans les journaux ou même à la télévision grâce à tes recherches et à ton travail haha ! Je trouve très inspirant ton intérêt pour les questions de discrimination de genre et de sécurité des jeunes dans les espaces urbains et nocturnes. Je pense que ton travail pourrait avoir un réel impact social, surtout parce qu’il combine recherche, créativité et propositions concrètes pour améliorer la société.
Encore merci pour cette très belle lettre et pour toutes tes réflexions enrichissantes.
Avec toute mon amitié,
Alissa Chaibou Souley.